MedFriendly®








Chiari Malformation
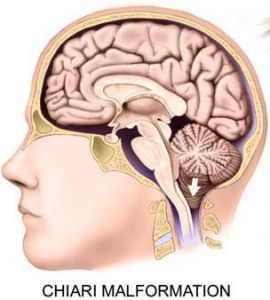
Chiari (pronounced key-ar-ee) malformation is a
condition in which important parts of the back, bottom
part of the brain are forced out of place in a downwards
direction through the opening in the bottom of the skull.
This opening is where the brain joins the spinal cord.
Thus, these structures in the back, bottom part of the
brain push down into the upper part of the spinal cord,
much like how a cork is pushed down into the neck of a
bottle.
The brain structures that extend downwards in Chiari
malformation are the cerebellar tonsils, the pons, and
the medulla oblongata.
FEATURED BOOK: Conquer Chiari: A Patient's Guide to Chiari Malformation
The cerebellar tonsils are two structures at the bottom part of the cerebellum. The
cerebellum is an area in the back, bottom part of the brain that plays an important role in
movement and coordination. The pons is very important for sleep and arousal and the
medulla oblongata is extremely important for controlling breathing. The cerebellum, pons,
and medulla oblongata tend to get longer and flatter in people with Chiari malformation.
In Chiari malformation, the cerebellar tonsils, pons, and medulla oblongata stick out
because there is not enough room at the back of the brain. Normally, the cerebellum,
pons, and medulla oblongata rest in an indented area of bone in the lower, back part of
the skull known as the posterior cranial fossa.
"Where Medical Information is Easy to Understand"™
However, the posterior cranial fossa is abnormally formed in people
with Chiari malformation, providing less space for these important
brain areas. With less space to be in, these areas of the brain are
crowded together and push downwards into the spinal cord.
ARE THERE DIFFERENT TYPES OF CHIARI MALFORMATION?
Yes. There are four different types of Chiari malformation. The four
different types are based on how severe the condition is. The
severity of the condition is based on how much the back parts of the
brain are pushing downwards. The types of Chiari malformation are
listed below:
TYPE 1: In this type, which is the most mild, the tonsils of the cerebellum (see above) have sunk down
from their normal position into the opening in which the spinal cord is located. In Type1 Chiari
malformation, the brainstem does not get longer. The brainstem is the pons, medulla oblongata, and the
midbrain, all of which are pictured above. The previous section described the medulla and the pons. The
midbrain is an area located above the pons that helps in breathing, and contains structures necessary for
hearing and vision.
Most children who do not have spina bifida have a Type I Chiari malformation. Spina bifida is a birth
defect in which part of the bones that surround the spinal cord do not form properly, leaving part of the
spinal cord exposed. Type 1 Chiari malformation usually presents in teenagers and adults.
TYPE II: When people refer to Arnold Chiari malformation, they are usually referring to Type II Chiari
malformation. This is the classic type of Chiari malformation. Not only are the cerebellar tonsils sticking
downwards out of position, but so are the various parts of the brainstem (see above), the cerebellar
vermis, and the fourth ventricle. The vermis of the cerebellum is a wormlike appearing structure in the
middle of the cerebellum. The vermis plays an important role in controlling the posture and tension of
muscles. The fourth ventricle is an area in the bottom, back part of the brain that connects the ventricles
in the cerebrum (the upper part of the brain) through a narrow canal called the cerebral aqueduct. The
cerebrospinal fluid comes through the fourth ventricle to bathe and cushion the outside of brain and spinal
cord.
TYPE II: When people refer to Arnold Chiari malformation, they are usually referring to Type II Chiari
malformation. This is the classic type of Chiari malformation. Not only are the cerebellar tonsils sticking
downwards out of position, but so are the various parts of the brainstem (see above), the cerebellar
vermis, and the fourth ventricle. The vermis of the cerebellum is a wormlike appearing structure in the
middle of the cerebellum. The vermis plays an important role in controlling the posture and tension of
muscles. The fourth ventricle is an area in the bottom, back part of the brain that connects the ventricles
in the cerebrum (the upper part of the brain) through a narrow canal called the cerebral aqueduct. The
cerebrospinal fluid comes through the fourth ventricle to bathe and cushion the outside of brain and spinal
cord.
Type II Chiari malformation is almost always associated with a meningomyelocele. Meningomyelocele is a
condition in which the spinal cord and its coverings stick out through an incorrectly formed area in the
bones that are supposed to surround the spine. These bones are known as the vertebral column.
Meningomyelocele condition tends to occur in the lower back. Other abnormalities can occur along with
Type II Chiari malformation, such as heart problems, absence of an anus (the area that poop comes out
of), and abnormalities of the stomach, urinary tract, and intestines. The urinary tract is the part of the body
that deals with the formation and release of urine. The intestine is a tube shaped structure that is part of
the digestive tract. It stretches from an opening in the stomach to the anus and occupies most of the
lower parts of the belly.
TYPE III: In this type, which is the most serious, the cerebellum has bulged through the area that is
supposed to contain it. The cerebellum sinks down into the opening in which the spinal cord is located and
can form an occipital encephalocele. An occipital encephalocele is a sac-like structure, containing brain
matter that sticks out of the back of the head. A sac-like structure containing brain matter can also form
that sticks out of the back of the neck. The brain matter inside of the sac consists of parts of the
cerebellum and the brainstem. A meningocele can also form, which is when the coverings of the brain or
spinal cord stick through an abnormal opening in the skull or stick through the bones that surround the
spine.
TYPE IV: Type IV Chiari malformation is associated with an underdeveloped cerebellum.
IS CHIARI MALFORMATION ASSOCIATED WITH ANY OTHER CONDITIONS?
Sometimes, Chiari malformation is associated with other conditions. For example, the pressure of the
back, bottom brain structures onto the spine can prevent the normal flow of cerebrospinal fluid. This can
cause the cerebrospinal fluid to flow into the spinal cord, leading to the formation of long, fluid-filled spaces
in the spine. This condition is known as syringomyelia. Syringomyelia is a rare condition in which long,
fluid filled spaces are present in the central gray matter (a gray looking substance) of the spinal cord and
surrounded by thick tissues made of glial cells. Glial cells maintain and support other cells. A cell is the
smallest, most basic unit of life, that is capable of existing by itself.
A condition similar to syringomyelia that is present in Chiari malformation is hydromyelia. Hydromyelia is
an increase in cerebrospinal fluid in the long, hollow tube that runs the length of the center of the spinal
cord. This tube, which is known as the central canal, becomes widened in hydromyelia. In hydromyelia,
there is no loss of spinal cord tissue. Instead, the spinal cord tissue becomes compressed (pushed
together) from the inside due to the pressure caused by buildup of fluid. Hydromyelia causes many of the
signs and symptoms (see below) of Type I Chiari malformation.
The crowding together of the brain structures in Chiari malformation can block the normal flow of
cerebrospinal fluid. This blockage can lead to an abnormal buildup of cerebrospinal fluid in the head, a
condition known as hydrocephalus. Cerebrospinal fluid is the cushiony fluid that protects the brain and
spine. It should be noted that hydrocephalus can make the abnormalities of the brain structures in Chiari
malformation worse. Syringomyelia, hydromyelia, and hydrocephalus are associated with Type I, II, and III
Chiari malformation. Hydromyelia is more commonly associated with Type II Chiari malformation than
Type I Chiari malformation.
Another abnormality associated with Chiari malformation is spina bifida and meningomyelocele. Spina
bifida is a birth defect in which part of the bones that surround the spinal cord do not form properly, leaving
part of the spinal cord exposed. Spina bifida is typically associated with Type II and Type III Chiari
malformation. Meningomyelocele is a condition in which the spinal cord and its coverings stick out through
an incorrectly formed area in the bones that are supposed to surround the spine. These bones are known
as the vertebral column. Finally, Chiari malformation is also associated with mental defects.
WHAT ARE THE SIGNS AND SYMPTOMS OF CHIARI MALFORMATION?
The abnormal pushing downwards of structures in the back, bottom part of the brain can lead to various
vomiting, stiffness, difficulty swallowing (a condition known as dysphagia), infections of structures that
help in breathing, gagging, muscle weakness in the head and face, strange feelings in the arms and legs,
and various degrees of mental impairment. These signs and symptoms usually begin in infancy, but may
not occur until the teenage years or early adulthood. The signs and symptoms of Chiari malformation are
often made worse when the person strains.
When people with Chiari malformation do not have symptoms in childhood, as they grow older they may
show signs of worsening brain impairment when they are teenagers and adults. Signs of such brain
impairment would be involuntary, rapid downward eye movements, in addition to double vision, dizziness,
headache, deafness, ringing in the ears, inability to coordinate movements, and episodes of sudden pain
around the eyes.
Teenagers with Type 1 Chiari malformation (see above) usually present with loss of pain and temperature
sensations in the arms and upper part of the body below the head, loss of muscle strength in the hands
and arms, and loss of movement and sensation in the arms that leaves the arms in a flexed position.
Adults with Type I Chiari malformation usually complain of neck pain, arm pain, and a headache at the
bottom of the skull that is made worse by coughing.
Signs and symptoms of Type II Chiari malformation are usually present soon after birth and could include
short periods in which breathing stops, a decreased ability to gag when something is stuck down the
throat, loss of arm strength, and involuntary and rapid downward eye movements.
Untreated Chiari malformation can lead to the formation of long-fluid filled openings in the spine, which can
further injure the person's spinal cord and function. If Chiari malformation goes untreated, it can lead to
worsening weakness in the arms and legs due to its effects on the spinal cord. In the worst-case
scenario, Chiari malformation can cause a lack of sensation or movement in the body due to its effects on
the spine.
WHAT CAUSES CHIARI MALFORMATION?
As was mentioned in the beginning section, the lower, back part of the skull (known as the posterior
cranial fossa) is abnormally formed in people with Chiari malformation. This abnormal formation provides
less space for these important brain areas. With less space to be in, these areas of the brain are
crowded together and push downwards into the spinal cord. The exact cause of these processes,
however, is unknown.
Some have suggested that Chiari malformation develops in the early formation of the cerebellum and
brainstem, when the baby is developing inside of the mother. There is very weak evidence that some
people develop Chiari malformation through the genes on their parents. Genes are units of material in a
person's cells that contain coded instructions as for how certain bodily characteristics (such as eye color)
will develop. All of a person's genes come from his/her parents. Some genes are normal whereas others
may be abnormal. Abnormal genes can cause diseases.
HOW IS CHIARI MALFORMATION DIAGNOSED?
Chiari malformation is diagnosed with a CT (Computerized Tomography) scan or Magnetic Resonance
Imaging (MRI) scans of the brain. CT scanning is an advanced imaging technique that uses x-rays and
computer technology to produces clear and detailed picture of the body area being examined. MRI scans,
however, are the best option to use for diagnosis of Chiari malformation. This is because MRI scans
produce extremely detailed pictures of the inside of the body by using very powerful magnets and
computer technology. MRI scans are more detailed, but more expensive than CT scans. It should be noted
that Chiari malformation is often misdiagnosed because it is a rare condition.
HOW IS CHIARI MALFORMATION TREATED?
The only treatment for Chiari malformation is surgery. When this is the case, the first step is to find a
neurosurgeon that specializes in Chiari malformation. A neurosurgeon is a doctor that operates on the
spine, brain, and/or nerves outside the brain and spine. The surgery is serious and not always 100%
successful. More than one surgery may be needed, but the patient is completely unconscious during each
surgery.
The surgery is done to reduce pressure inside the head by providing more space for the bottom of the
cerebellum, where it is pushing against the brain stem (see first section) and spinal cord. This is done by
removing a small part of bone at the bottom of the skull. In addition, the back part of the first and
sometimes additional bone sections around the spinal cord need to be removed. How far down the spinal
cord the surgeon needs to operate to remove bone, depends on how far down the brain matter has gone.
If the child has a build-up of cerebrospinal fluid (see above) or has long-fluid filled openings in their spine,
the surgery will be done in a different way so as not to cause further damage to the child.
During the surgery, the outer covering of the brain and spinal cord will be opened and tissue will be
attached to it to provide more room for the cerebrospinal fluid to flow. In some cases, to get rid of the
fluid-filled space, a flexible tube called a shunt can be placed inside of it. From here, the tube will drain the
extra fluid into chest or the space between layers that line the belly. The fluid will then be absorbed along
the wall of the belly. If surgery succeeds, it will usually stop the condition from getting worse and possibly
help to moderately decrease the symptoms. These surgeries can be done together or separately.
Surgery can also be done to repair a meningomyelocele. Remember that a meningomyelocele is a
condition in which the spinal cord and its coverings stick out through an incorrectly formed area in the
bones that are supposed to surround the spine. These bones are known as the vertebral column and the
abnormality in this area is what is corrected during the surgery.
Unfortunately, over time, surgery for Chiari malformation is not always successful and more than one
surgery may be needed. In cases in which surgery is not needed, the patient needs to be monitored often
by the treating doctor with physical examinations and scans of the brain and spine. Drugs are often used
to treat the symptoms of Chiari malformation, such as headaches.
WHAT IS THE PROGNOSIS OF PEOPLE WITH CHIARI MALFORMATION?
Most people with Chiari malformation will do well after surgery and have improvement in their signs and
symptoms. Many people with Chiari malformation go on to live with minimal symptoms. The more severe
the condition, however, the worse the prognosis. Infants with very severe forms of Chiari malformation
may have life-threatening complications.
DOES CHIARI MALFORMATION OCCUR MORE IN MALES OR FEMALES?
Chiari malformation occurs more often in females than males.
WHO IS CHIARI MALFORMATION NAMED AFTER?
Chiari malformation is named after Hans Chiari, a pathologist from Austria who lived from 1851-1916. A
pathologist is someone who interprets and diagnoses the changes caused by disease in tissues and body
fluids.
WHAT ELSE IS CHIARI MALFORMATION KNOWN AS?
Chiari malformation is also known as Arnold-Chiari malformation, Arnold-Chiari deformity, Arnold-Chiari
syndrome, Chiari's malformation, Chiari, and cerebellomedullary malformation syndrome.