MedFriendly®



Patellofemoral Arthralgia
Patellofemoral arthralgia is pain in the front of the knee.
However, the pain can also be felt behind and around
the kneecap. The pain is usually a dull ache which
becomes sharp during activities that increase pressure
over the kneecap. Examples of such activities include
squatting, running, going up and down stairs, and
sitting for extended periods.
IF THE KNEES MAKE A CLICKING SOUND OR
FEEL LIKE THEY ARE GIVING WAY, DOES THIS
INDICATE PATELLOFEMORAL ARTHRALGIA?
FEATURED BOOK: The Permanent Pain Cure for Joint Pain
A clicking sound when flexing and extending the knee is actually quite common in young
individuals and in and of itself, does not mean that one has patellofemoral arthralgia. It is
uncommon in patellofemoral arthralgia for one to have a sensation that the knee is
giving way. Such a sensation usually indicates more severe misalignment.
WHAT CAUSES PATELLOFEMORAL ARTHRALGIA?
Patellofemoral arthralgia is caused by irritation of surrounding structures such as the fat
pad, ligaments, or the retinaculum (a type of tendon). A ligament is a tough band of
bones.
"Where Medical Information is Easy to Understand"™
The irritation in patellofemoral arthralgia can have two possible
causes. The first is an abnormality in the structure of the knee or
supporting structures that causes abnormal tracking of the kneecap
during movement. Two examples of structural abnormalities include
weakness of the vastus medialis oblique muscle or tightness of the
medial (middle) or lateral (side) retinaculum (see above). The
vastus medialis is one of 4 parts of the quadriceps muscle. The
quadriceps muscle is a muscle with four distinct parts that is
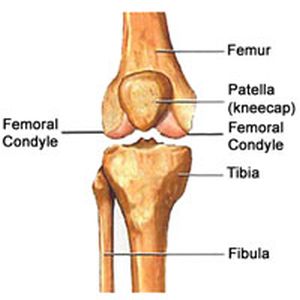
responsible for straightening the knee. The height of the femoral
condyles and the depth of the sulcus (groove) between them is
important in keeping the kneecap in place so that it tracks properly.
The femoral condyles are a large pair of prominences at the farthest end of each femur. The femur is the
long bone of the leg that runs from the hip to the knee. The femoral condyle is pictured above.
If the groove between the condyles is not deep enough or the facets of the kneecap are deformed,
patellofemoral arthralgia can result. Specifically, all of the structural abnormalities mentioned above can
cause too much pressure between the kneecap and femoral condyles during flexing and extending
movements.
The second possible cause of patellofemoral arthralgia is gradual wear and tear caused by tiny daily
repetitive stresses (overuse). A common activity leading to such overuse is running. When the pain
occurs at the area where the femur and patella join together (see above) the source is likely irritation of
the many nerves located in the subchondral bone (bone below the cartilage) of the patellae. This is
because cartilage does not have pain fibers. Cartilage is a type of soft, flexible tissue that helps form
many important body structures.
In some patients, soft tissue around the kneecap may be the source of the pain, especially in young
active patients where there is mild misalignment of the kneecap (also known as the patella). In these
cases, strain on tendons can produce inflammation and pain.
WHAT ARE COMMON CLINICAL FINDINGS IN PATELLOFEMORAL ARTHRALGIA?
When the physician squeezes the middle or side facets on the back surface of the kneecap, this may
cause pain. The physician may squeeze these facets while mildly displacing the kneecap to the middle or
the side. Squeezing the kneecap onto the femoral condyles may cause characteristic discomfort. When
both sides of the kneecap are grasped while the patient contracts the quadriceps muscle, the added
pressure of the kneecap against the femoral condyles may cause discomfort.
WHO GETS PATELLOFEMORAL ARTHRALGIA?
Patellofemoral arthralgia is common in people who regularly engage in competitive or recreational
activities. It is most common in adolescents and young adults. Females appear to be affected more than
males. This may be because females have a wider pelvis, which leads to an exaggerated Q angle. The
Q angle is the angle by which the quadriceps muscles pull at the knee. The Q angle is typically about 15
degrees in adults. Some have questioned the relevance of the Q angle in patellofemoral arthralgia.
WHAT IS THE DIFFERENCE BETWEEN PATELLOFEMORAL ARTHRALGIA AND
CHONDROMALCIA PATELLAE?
Chondromalacia patellae is a painful disorder of the knee in which the cartilage directly behind the
kneecap becomes soft and damaged. The type of cartilage affected in chondromalacia patellae is called
articular cartilage. The word "articular" means "referring to a joint." A joint is a place where two bones
contact each other. In most cases of patellofemoral arthralgia, the articular cartilage is not injured. There
is little evidence that untreated patellofemoral arthralgia leads to chondromalacia patellae.
Patellofemoral arthralgia may spontaneously resolve by itself although many patients have tried a wait
and see approach before pursuing treatment. One form of treatment is relative rest. The term relative
rest is used because it means that the person can still be active but should be doing non-impact aerobic
activities that do not risk injuring the knee.
In addition to relative rest, physical therapy is commonly recommended, with special emphasis placed
upon strengthening the quadriceps muscle. Stretching exercises are also used. The decision of which
exercises to perform depends on an accurate physical examination. Twenty minutes of physical therapy
a day is considered reasonable by many. Symptom improvement with exercise may take up to 6 weeks.
Yet another form of treatment includes using a different quality of shoe, with the major factor being that
the shoe is not worn out. For example, some runners change their shoes every 300-500 miles. Arch
supports or custom made foot inserts may be helpful and are fairly inexpensive.
Ice is sometimes used to reduce inflammation, especially after activity. This is usually accomplished by
placing an icepack over the knee and holding it in place with an elastic band. Other options include a
frozen gel pack, crushed ice in a plastic bag, or a bag of frozen vegetables. Some people try non-
steroidal anti-inflammatory drugs (known as NSAIDs), but there is no proven benefit from this and there
is always the concern of side effects.
Some people use knee sleeves or knee braces to stabilize the kneecap. However, the use of such
devices is controversial since it has not been proven to work and is not considered a substitute for
physical therapies. Some people tape the kneecap to keep it stable. This may offer short term pain relief.
Most physical therapists are trained in taping methods and can teach patients how to do this themselves.
Most patients do well with non-surgical forms of treatment, especially if they are disciplined. Surgery for
patellofemoral arthralgia is only used as a last resort. Surgery involves cutting the lateral (side)
retinaculum to decrease the amount that the kneecap is pulled to the side. This type of surgery is known
as lateral release.
WHAT ELSE IS PATELLOFEMORAL ARTHRALGIA KNOWN AS?
Patellofemoral arthralgia is also known as retropatellar pain syndrome, patellofemoral pain syndrome,
extensor mechanism disorder, lateral patellar compression syndrome, patellalgia, and patellofemoral
dysfunction.
WHY IS IT CALLED PATELLOFEMORAL ARTHRALGIA?
Patellofemoral arthralgia comes from the Latin word "patella" meaning "kneecap," the Latin word femur
meaning thigh, the Greek word arthron meaning joint, and the Greek word "algos" meaning "pain."
Put the two words together and you have "kneecap thigh joint pain."